Breasts and nipples come in many shapes and sizes, and most work well for breastfeeding. If one or both of your nipples are flat or inverted, getting started may take a little extra time and patience, but there are many ways to help your baby breastfeed.

Summary
- Nipples come in a wide range of shapes and sizes, and most work well for breastfeeding.
- Learning about breastfeeding and seeing it in action before your baby is born can be very helpful. There is no evidence that treating inverted nipples during pregnancy helps.
- After birth, hold your baby skin-to-skin to stimulate their feeding reflexes.
- If your baby doesn’t start breastfeeding straight away, don’t panic. Express your milk to keep your baby well fed and protect your milk supply.
- There are many ways to help babies start breastfeeding. Time, patience, and support from a breastfeeding helper are often all that’s needed.
- Pumps and other devices to pull out inverted nipples might be worth a try.
- Whatever feeding looks like for you and your baby, we’re here to support you.
On this page
Preparing for breastfeeding – what really helps
Your baby arrives – getting off to a good start
If your baby doesn’t start breastfeeding straight away
What are inverted nipples?
An inverted nipple is one that turns inward instead of pointing outward. One or both of your nipples may be inverted.
Most nipples that look inverted ‘at rest’ will protrude when stimulated. If you think yours might be inverted, try placing your thumb and finger on opposite sides of the areola (the darker area of skin surrounding the nipple) and squeezing gently inwards. (1)
A nipple that stands out when stimulated like this is not fully inverted. Some nipples are partly inverted, looking dimpled or folded. A true inverted nipple that can’t protrude at all is quite rare. These severely inverted nipples (sometimes called ‘Grade 3’) retract deeply when compressed or stimulated.
Flat nipples are exactly what they sound like – they don’t stick out much or at all at rest, but they extend when stimulated.
Why is my nipple/are my nipples like this?
Nipples may be inverted because of:
- Less dense connective tissue beneath the nipple, compared to protruding nipples.
- Short milk ducts.
- Tight fibrous bands of connective tissue pulling the centre of the nipple into the inner breast tissue. [2]
Most people with inverted nipples have always had them, though nipples can sometimes become inverted after surgery or disease affecting the breast. (3) If your nipple has unexpectedly become inverted when it wasn’t before, let your doctor know.
Preparing for breastfeeding – what really helps
There’s no evidence that treating nipples during pregnancy helps with breastfeeding. An early ‘diagnosis’ of flat or inverted nipples may even make it harder, by undermining your confidence. (4, 5) It’s common for nipples to change shape during pregnancy, gradually protruding more.
There are lots of other things you can do before your baby is born, to help get ready for breastfeeding:
- Learn as much as you can about breastfeeding. Reading this piece is a great start! You might also enjoy our free Beginning Breastfeeding online course and our handbook, The Art of Breastfeeding (9th edition, 2024).
- Spend time around breastfeeding mothers and babies before your baby arrives, and make contact with your local LLL group. You are very welcome to attend LLL Meetings before and after birth.
- Learn how to express your milk. Find out how to express by hand and how to pump, store and handle milk. If you know how to express your milk, you can:
- soften a full, tight breast, which might help your nipple stand out more,
- give your baby a little milk to encourage them to breastfeed, and, if necessary
- keep your baby fed and protect your milk supply while you work towards breastfeeding.
You might like to try expressing your colostrum in the last few weeks of pregnancy. Any colostrum you collect can be frozen and given to your baby after birth if needed.
Your baby arrives – getting off to a good start
Many babies have no difficulty feeding when their mother has flat or inverted nipples, so start off by putting your baby to the breast and see what happens.
Holding your baby skin-to-skin as soon as possible after birth is the best way to get breastfeeding started. (6, 7) Placed tummy-down with their hands and feet on your body, newborns have many hard-wired reflexes that help them find the breast and latch on.

‘Laid-back’ positions make the most of your baby’s inbuilt feeding instincts, as well as being comfortable for you. Babies often lick the nipple or touch it with their hands to stimulate it before latching on – they can do this easily in laid-back positions. Your baby might surprise you by crawling up to the breast and latching with very little help!
Skin-to-skin isn’t just for the first few hours – it’s a lovely way to get to know your baby and practise breastfeeding in the weeks ahead.
The importance of good attachment
Whatever breastfeeding specialists think about different treatment options for inverted nipples (see below), all agree that getting a deep latch is crucial. (8)
Babies breastfeed, not nipplefeed. With a large enough mouthful of breast, your baby can nurse effectively, whatever kind of nipples you have.
Our articles on comfortable breastfeeding and positioning and attachment have lots of information on how to help your baby attach deeply.
If your baby doesn’t start breastfeeding straight away
It takes some babies a while to get going. Don’t panic – as long as your baby is fed, and you’re building your milk supply, you’ve got plenty of time to work towards breastfeeding.
Hand express or pump your breasts to bring in plenty of milk. Aim to express 8-12 times in 24 hours, as often as a healthy newborn would usually nurse.
You may want to avoid using artificial teats (bottles or dummies) at this stage. Babies are strongly ‘hardwired’ to breastfeed and usually aren’t easily put off, but things can be more challenging if you have flat or inverted nipples. Babies rely on a series of cues to recognise the breast. When they feel a nipple against their face, they turn towards it. Feeling a nipple towards the back of their mouth helps trigger sucking. When nipples are flat or inverted, these cues can be harder for a baby to pick up. If your baby gets used to the feel of a firm silicone teat, it may make it harder for them to recognise your nipple and latch on. (9) Once your baby has started breastfeeding, over time they learn that the nipple is there even if they can’t feel it.
Your expressed milk could be offered in other ways, such as by cup while you work towards breastfeeding. This video shows how to cup feed a young baby. You can read about a range of feeding tools here. A breastfeeding helper can support you to find a feeding method that suits you and your baby.
Tips for encouraging your baby to breastfeed
Pick your moment
Keeping your baby close – skin-to-skin on your chest, in your arms, or in a sling – helps you notice the early signs that they’re ready to feed. Small movements of the head, mouth, or hands are your cue to offer the breast. When a baby isn’t too hungry yet, they usually have more patience to explore and practise latching.
Use expressed milk
If your baby doesn’t latch at first, a little expressed milk can help. You could:
- rub a few drops over your nipple and areola. The smell of milk may help your baby find and recognise the nipple. Licking helps your nipple protrude and encourages your baby to latch.
- try ‘drip-drop feeding’. Have a helper drip milk down your breast from a spoon, dropper, or syringe. It’s messy, but sometimes it works!
- offer a small amount of expressed milk by spoon or cup to take the edge off your baby’s appetite, before trying again.
- offer a whole feed of expressed milk – your baby might latch more easily when they’re fed, calm, and ready to snooze.
Soften your breast
Your nipples may appear flatter in the first few days after birth, because your breasts are engorged (swollen with extra fluid). A soft breast has more ‘give’, allowing the nipple to protrude as much as it can. Breastfeed or express frequently to keep the breast soft.
You can find more information in our article on engorgement.
You could also try reverse pressure softening just before a feed, to move fluids away from the nipple area. (10)


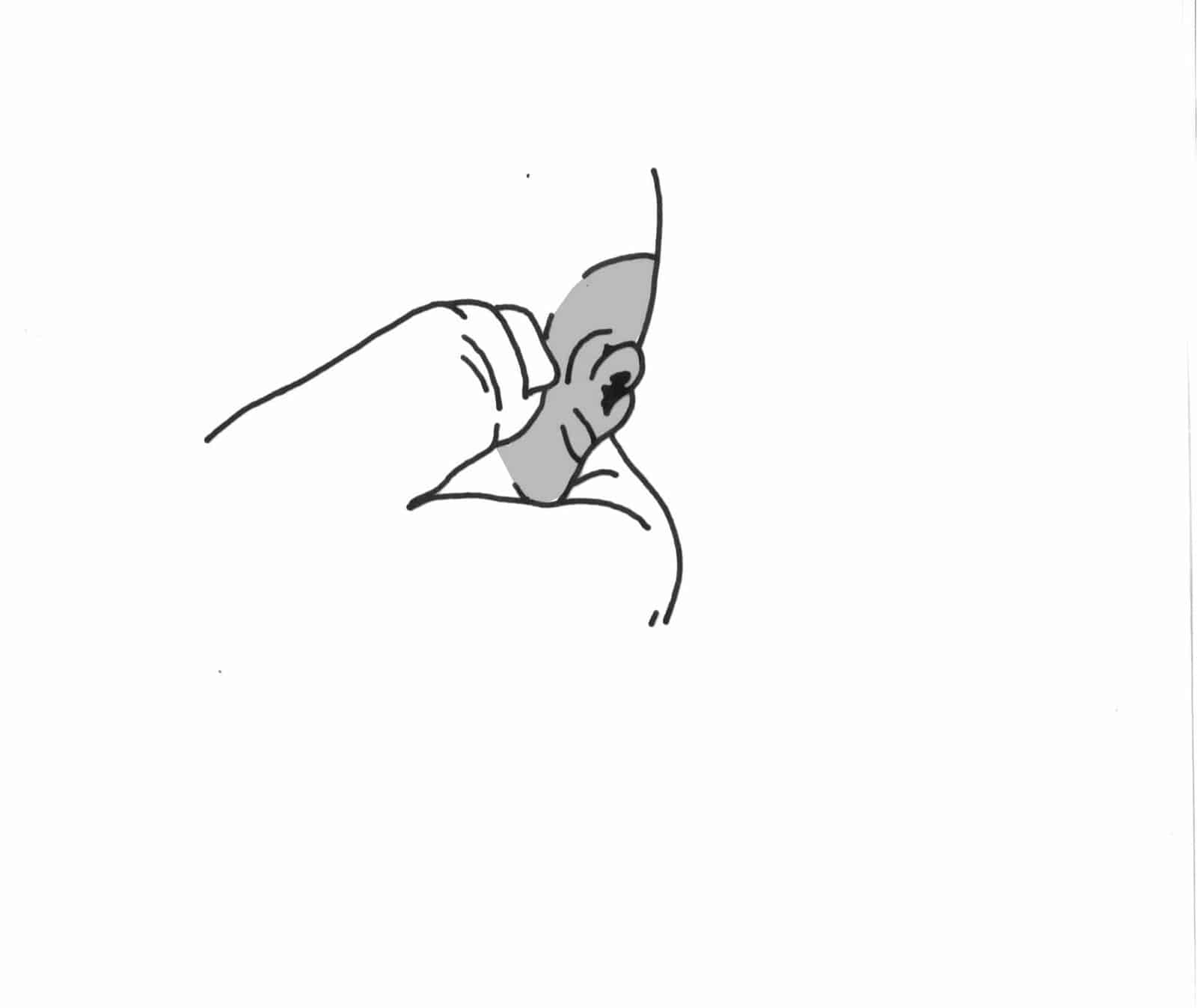
Pictures: Reverse pressure softening
Apply gentle steady pressure with your fingertips on the areola around your nipple for about a minute to move fluid away from the base of the nipple. You can also press with the sides of your thumbs or fingers.
You can see a video here.
Stimulate your nipples
You could try:
- rolling your nipple gently between your thumb and finger
- a ‘nipple nudge’ – use your finger to push up into the breast from underneath and help push your nipple out further
- touching your nipple with a cold wet cloth
- pulling back on the breast tissue to help the nipple protrude
Shape the breast
Try the ‘breast sandwich’ – compress your breast like you would a big sandwich, in line with your baby’s mouth. This can help them grasp more breast tissue. It doesn’t matter if your fingers are closer to the upper jaw, but try to keep the ‘lower jaw fingers’ out of your baby’s way.
You can find more information about how to help your baby latch deeply in our article Comfortable Breastfeeding: Essentials.
Work with your baby’s preferences
It’s common for babies to have a ‘favourite’ breast, even without inverted nipples. When nipples are very different, babies may show a strong preference for one side.
- You might be able to encourage your baby to breastfeed on their less preferred side by offering it first, when they are hungrier, or when they’re in light sleep. You could express that breast as well, to keep milk production high – this may give your baby more incentive.
- However, some babies are quite determined in their preferences and end up breastfeeding from only one side. It is possible to feed a baby exclusively from one breast – many mothers breastfeed twins (or more!), or nurse after a single mastectomy. Milk production operates independently in each breast, so it’s possible to maintain a full supply on one side while the other gradually stops producing. Or you might partially breastfeed; nurse on one side and also use some donor milk or formula.
Try using a breast pump
With some inverted nipples, when a baby tries to breastfeed, they compress the buried nipple beneath the areola. If simpler techniques of stimulating your nipples don’t help, you could try using a breast pump to draw the nipple out before a feed. Once may be enough, or you may need to pump before each feed for a few days or weeks.
Nipple shields
A nipple shield is a thin piece of shaped silicone that fits over the areola and nipple during feeds. For some babies, a shield can make it easier to recognise and latch onto a flat or inverted nipple. If your baby is still struggling to latch using the suggestions above, a nipple shield may be worth trying.
One possible drawback is that, if it helps, your baby may find it harder to latch without the shield. However, if you’re comfortable using a shield, and it’s working well for your baby, this isn’t a problem. Most babies who need shields to get started can eventually nurse without them.
Shields, like nipples, come in many shapes and sizes, and you might need to try a few sizes or styles to find what works best for you. If you can, work with a breastfeeding helper who is experienced with shields. They can help you find a good fit, and make sure the shield is applied properly. If your baby will latch, your breastfeeding helper can work with you to make sure they’re breastfeeding effectively.
Look after your nipples
You may experience some discomfort in the first couple of weeks of breastfeeding as your baby gradually draws your nipple out.
This is temporary, and different from nipple damage and soreness caused by a baby who isn’t latching on well. It may be caused by bands of tissue that hold the nipple in stretching or breaking, or by damp skin becoming chapped, when the nipple tucks itself away. (11)
It might help to:
- pat your nipple dry and apply a small amount of a simple barrier ointment (such as petroleum jelly) immediately after a feed
- replace breast pads frequently, and change wet bras
Treating inverted nipples
Various techniques and devices can be used to draw out nipples. Research has not shown any of them to have clear benefits, but if the measures suggested above aren’t enough, you might like to give one or more of these a try. (12, 13)
The Hoffman Technique
This is a gentle manual nipple-stretching technique that some mothers find helpful after birth. (14) With a thumb on each side of the base of the nipple, press in firmly against the breast tissue and at the same time pull your thumbs away from each other. If this feels comfortable, repeat five times each morning, moving your thumbs around the base of the nipple. If it hurts, this technique may not be appropriate for you.
Devices to draw out the nipple
There are lots of products designed to be worn between feeds, or used immediately before a feed, to help draw out the nipple.
Breast shells
A breast shell has two parts: a dome, and a snap-on backing with a hole that fits around the nipple. The shell is worn inside a bra, applying steady pressure on the areola to try and draw out the nipple. Some mothers find them helpful, but it’s important to be aware that they can increase the risk of mastitis. If you decide to try breast shells, it’s recommended to wear them for no longer than 30 minutes before a feed. You may need to wear a bra with a larger cup size than normal. (15)
Breast shells need to be washed daily. Any milk collected should be discarded because of high levels of bacterial growth, compared with freshly expressed milk.
Nipple everter devices are used immediately before a feed, to make the nipple more prominent and graspable. There are several kinds:
- Some have a squeezy bulb to generate suction on the nipple
- Others are like soft cups, placed over the nipple and gently squeezed, creating suction to draw the nipple out
- Syringe-type everters – you apply one end to your nipple and pull out the plunger
If using devices, it is important to follow the manufacturer’s instructions, and you may wish to consult a breastfeeding specialist.
Getting the help you need
It can be frustrating when it takes longer to get started with breastfeeding than you expected. Most babies will get there eventually – sometimes with a few tips and tricks, like the ones above. You can find more ideas in our article My Baby Won’t Breastfeed.
If your baby has extra challenges, such as being born prematurely or having health complications, even more time and patience may be needed. A premature, tongue-tied baby, for example, may find it harder to deal with flat or inverted nipples than a full term baby with normal tongue mobility. How ‘stretchy’ your breast tissue is also plays a part. Both of you are doing the best you can. Whatever feeding ends up looking like for you, we’re here to support you all the way.
Written by Karen Butler, Sue Upstone & mothers of LLLGB.
Updated by Nicola Coles-Carr, Jayne Joyce, and Charlotte Allam, February 2026.
Review date: February 2029.
If this article has helped you, please consider supporting LLLGB with a donation. Every gift, however small, helps keep breastfeeding information and support flowing.
Further Reading
From our website
Antenatal Expression of Colostrum
Beginning Breastfeeding
Bottles and other tools
Comfortable Breastfeeding
Engorged breasts – avoiding and treating
Exclusively expressing your milk
Getting back on track after a difficult start
Is My Baby Getting Enough Milk?
Nipple pain
Nipple ShieldsPositioning and Attachment
Using donor milk or formula to support breastfeeding
From LLLI
Inverted and flat nipples
Other Websites
Books
The Art of Breastfeeding. La Leche League International, 9th edition, 2024.
References
- Mohrbacher, Nancy. Breastfeeding Answers: A Guide for Helping Families. 2nd ed., Praeclarus Press, 2020, p. 739.
- Terrill, P J, and M J Stapleton. “The inverted nipple: to cut the ducts or not?.” British journal of plastic surgery vol. 44,5 (1991): 372-7. doi:10.1016/0007-1226(91)90152-a. Available at https://www.jprasurg.com/article/0007-1226(91)90152-A/pdf (accessed 20th October 2025).
- Nagaraja Rao, D., and R. Winters. “Inverted Nipple.” StatPearls, StatPearls Publishing, updated 4 July 2023. Available at www.ncbi.nlm.nih.gov/books/NBK563190/ (accessed 22 December 2025)
- Alexander, J M et al. “Randomised controlled trial of breast shells and Hoffman’s exercises for inverted and non-protractile nipples.” BMJ (Clinical research ed.) vol. 304,6833 (1992): 1030-2. doi:10.1136/bmj.304.6833.1030. Available at https://pmc.ncbi.nlm.nih.gov/articles/PMC1881748/ (accessed 23 December 2025).
- “Preparing for breast feeding: treatment of inverted and non-protractile nipples in pregnancy. The MAIN Trial Collaborative Group.” Midwifery vol. 10,4 (1994): 200-14. doi:10.1016/0266-6138(94)90055-8.
- Moore, Elizabeth R., et al. “Immediate or Early Skin-to-Skin Contact for Mothers and Their Healthy Newborn Infants.” Cochrane Database of Systematic Reviews, vol. 2025, no. 10, Oct. 22 2025, Art. no. CD003519, doi:10.1002/14651858.CD003519.pub5. Available at https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003519.pub5/full (accessed 23 December 2025).
- Widström, Ann-Marie et al. “Skin-to-skin contact the first hour after birth, underlying implications and clinical practice.” Acta paediatrica (Oslo, Norway : 1992) vol. 108,7 (2019): 1192-1204. Available at https://pmc.ncbi.nlm.nih.gov/articles/PMC6949952/ (accessed 23 December 2025)
- Blair, Anna et al. “Predictors of Effective Breastfeeding in Newborns and 6-Week-Old Infants: Modifiable Pre-Feeding, Positioning and Latching-On Elements.” Acta paediatrica (Oslo, Norway : 1992) vol. 114,12 (2025): 3317-3324. doi:10.1111/apa.70261. Available at https://pmc.ncbi.nlm.nih.gov/articles/PMC12599608/ (accessed 23 December 2025).
- Wilson-Clay, Barbara, and Kay Hoover. The Breastfeeding Atlas. LactNews Press, 2017, p. 47.
- Cotterman, K Jean. “Reverse pressure softening: a simple tool to prepare areola for easier latching during engorgement.” Journal of human lactation : official journal of International Lactation Consultant Association vol. 20,2 (2004): 227-37. doi:10.1177/0890334404264224
- Mohrbacher, Nancy. Breastfeeding Answers: A Guide for Helping Families. 2nd ed., Praeclarus Press, 2020, p. 741.
- Kaya, Özge et al. “The effect of interventions on flat and inverted nipple on breastfeeding: A systematic review.” Journal of pediatric nursingvol. 74 (2024): e1-e13. doi:10.1016/j.pedn.2023.07.024. Available at https://www.pediatricnursing.org/article/S0882-5963(23)00202-6/abstract (accessed 21 December 2025).
- Belal, Ghada Abd El-Salam, and Ekbal Ebrahim Abdelmenem. “Effect of Nursing Interventions Strategies for Inverted Nipple on Efficiency of Early Breastfeeding among Primiparous Mothers.” Assiut Scientific Nursing Journal, vol. 12, no. 45, July 2024, pp. 341–358. doi:10.21608/asnj.2024.306764.1868. Available at https://journals.ekb.eg/article_378058_e4ea8a75adf4de4334b334c7d4197f2b.pdf (accessed 21 December 2025).
- Thurkkada, Anju Philip et al. “Effectiveness of Hoffman’s Exercise in Postnatal Mothers With Grade 1 Inverted Nipples.” Journal of human lactation : official journal of International Lactation Consultant Association vol. 39,1 (2023): 69-75. doi:10.1177/08903344221102890
- Mohrbacher, Nancy. Breastfeeding Answers: A Guide for Helping Families. 2nd ed., Praeclarus Press, 2020 p. 739.
Copyright LLLGB 2016, 2026