You may be reading this because you have a preterm baby, or because you are expecting to deliver your baby before full term and you want to be prepared. Perhaps you’re supporting someone who has recently had a preterm baby. Whatever your situation then we hope this information will help to get breastfeeding off to a successful start.
Before your baby arrives
Your premature newborn
Establishing breastfeeding
Looking after your own health and wellbeing
Taking your breastfed baby home
Before your baby arrives
If you know your baby will be arriving soon, you may wish to try antenatal expression of colostrum. This is where you hand express some of the thick, creamy first milk into a sterile container such as a syringe. This can be given to your baby immediately after birth reducing the possibility of them needing to have early formula feeds. Hypoglycaemia (low blood sugar) can cause serious long term health problems if left untreated, and preterm babies are at higher risk of low blood sugar than babies born at term. Having some colostrum ready means that this is available instead of formula (or donor milk if available).
If you are at risk of early labour and taking precautions to avoid it, then consult with your healthcare professionals about your individual case before starting antenatal expression as it may be considered to increase your risk of going into labour.
You can read more about antenatal expression here.
If there is time before your baby arrives, someone from the paediatric team on the neonatal unit where your baby will be cared for should come and talk to you about how you plan to feed your baby. You can supply them with any expressed colostrum you have in a labelled container, and discuss how you wish your baby to be fed while you are establishing your milk supply.
Some neonatal units will have access to donor breastmilk, and will be able to tell you if your baby will be eligible to receive this – as supply is limited, this is likely to be restricted to the babies who need it the most. They will discuss and get your consent if formula may need to be given while you are building your milk supply. This may also be the time to talk about how you want supplementary feeds to be given to your baby.
Smaller or weaker babies will be given a nasogastric tube, to allow milk (your own, donor or formula) to be fed down the tube. Bigger and stronger babies may be given bottles. You may wish to discuss paced bottle feeding (the art of giving bottle feeds in a way that supports breastfeeding) or cup feeding.
If you wish to express breastmilk for your baby, then your hospital should be able to provide you with a breastpump – asking for this before your baby is born means that you have it ready as early as possible. In the early days you need to be stimulating milk production in your breasts between eight and twelve times in twenty four hours, including at least once at night – this might be by your baby feeding effectively at the breast, or pumping sessions.
To read more about successfully expressing breastmilk, click here.
Your premature newborn
When you baby arrives there is likely to be a sudden rush of activity as your baby is checked and stabilised. They may be rushed off to the neonatal unit leaving you feeling stranded in the delivery unit. Be kind to yourself. You may feel that starting to express milk is a practical way that you can be involved in their care even when you are apart from each other. There is evidence to show that if you start expressing within the first hour after birth it can have a long term positive effect on your milk supply.
Establishing breastfeeding
You may be expressing on your ward (if you are still an inpatient) or on the neonatal unit. Many mothers find that being close to their babies while they are expressing can help to increase the amount that they are able to express. If you are separated, looking at photos of your baby can help or smelling something that has been close them.
If you are expressing on the unit, you may wish to be close to your baby as you do so. Some mothers use screens for privacy. You can ask for these to be provided. You don’t have to use screens if you prefer not to – using scarves or nothing at all is a completely acceptable choice. Do what you feel comfortable with and helps your milk to flow easily. Listening to music may help you to relax and increase your milk production.
You are the person most known and familiar to your baby. Being with you is the safest and most secure they can possibly feel. If your baby is very fragile they may not be able to come out of their incubator at first. Ask the staff how you can be involved in their care and to show you how to hold and comfort them through the vents in the incubator. Once your baby is able to come out of the incubator, then kangaroo care can become an important part of your time together. This is where your baby is placed skin to skin on your chest for as long as possible and a blanket put over both of you. Your baby is able to enjoy the sensations of your closeness and the deep relaxation and comfort they feel helps them to regulate their breathing, temperature and other health indicators. It also helps your breast to become a familiar environment and allows them to practise feeding directly from the breast easily.
It used to be thought that babies under a certain gestation didn’t have the ability to suck and swallow, or that directly breastfeeding was tiring to them. Happily, more recent studies have disproved these concerns. Once babies are well enough to breathe unaided (off ventilation and continuous positive airway pressure – CPAP), they can be brought to the breast. Smaller and younger babies will still need to have some of their milk given to them via tube feeds, but this allows you and your baby to learn to breastfeed together without a feeling of pressure.
Smaller babies have smaller mouths and lower muscle tone. This may mean you need extra support to get breastfeeding established. Seek skilled help early and often. Keep asking until you find someone who is able to support you effectively.
Premature babies often find it easier to feed in laid back breastfeeding positions. This is where you are supported in a reclined position with your baby tummy down on top of you. This helps gravity to ‘stick’ your baby to you and stops them slipping off. If you need to sit in a more upright position, then supporting the whole length of your baby’s body close to yours with a hand behind their shoulders means they don’t have to support their weight and stops them from curling in on themselves. Read more about laid back breastfeeding here.
You may find that your baby quickly falls asleep when breastfeeding. This isn’t a sign that you are exhausting them, but that they are small and being soothed. You can help them to stay awake for longer by washing their face with cool water, gently blowing on them or tickling their feet. You may find that breast compressions – gently smoothing down your breast towards the nipple – helps your baby to stay alert and interested in feeding as this makes the milk flow more quickly and easily for them.
All new babies need to feed frequently – and premature babies are no different. The volume of milk that their stomachs can take at each feed is very small, and breastmilk is easily digested. It is normal for babies to feed between 8-12 times in a 24 hour period, including at least once at night.
Neonatal unit staff need to be able to ensure that all the babies in their care are receiving the right amount of milk for them to grow. Premature or sick babies may be less able to communicate their need for milk. These two things combined mean that units often use feeding schedules, with feeds timetabled every two, three, or even four hours.
When you agree how often your baby is to be offered supplemental feeds (any milk not directly from the breast) it may be helpful to remember that four hourly is less frequently than you would expect a healthy, full term newborn to feed. You may also choose to consider these as ‘backup’ feeds – any time spent feeding directly from the breast doesn’t reset the clock, but is bonus extra calories. Keep writing down how often you are breastfeeding in your baby’s notes, as this may help you and the staff to feel confident about the transition from scheduled, measured feeds, to baby led, responsive feeding.
One of the things the unit staff will look for in a baby coming close to going home is that your baby is able to rouse themselves to feed. If your baby is waking for feeds more often than their feeding ‘schedule’ (and you are spotting signs of effective feeding), this may be a sign that they are becoming better able to manage their own need for milk. You will probably need to keep offering more frequently than they ask for milk – this is true for many babies. Remember, you can’t feed too often, and your baby can always say no if they don’t want milk right now!
Breastmilk is an incredibly responsive food, made specially for each baby. The milk that you are making for your premature baby will be even more densely nutritious than the milk of a full term mother. Every drop of milk that you can supply for your baby is like medicine – strengthening and building their immune system and providing the calories they need to grow. Some mothers feel that providing milk for their babies is a unique way that they can care for their babies. It can be an important part of bonding with a new and fragile baby. While your baby will continue to benefit from your milk for as long as you provide it, you aren’t tied to expressing for longer than you want to do so. If you decide it’s time to stop, then gradually reducing your pumping sessions will slow and stop your milk production without causing problems for you.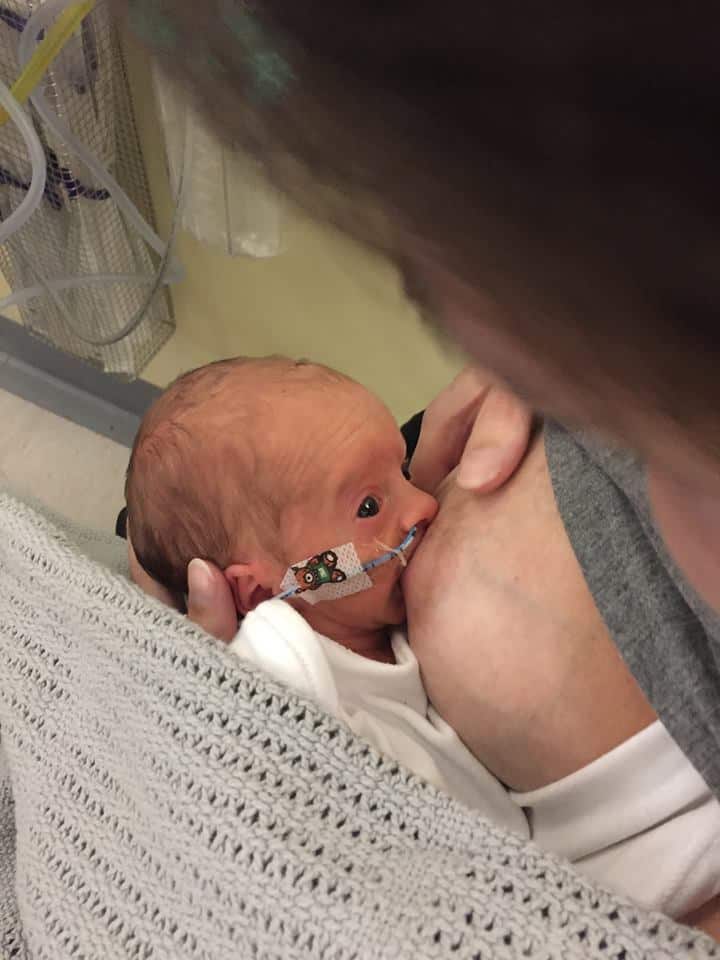
Looking after your own heath and wellbeing
You will be recovering from pregnancy and birth, and may be experiencing additional health problems. It is important to remember to look after yourself – the more smoothly your recovery goes, the more strength and energy you will have to become more and more involved in your baby’s care. If you have older children at home, you may be struggling to balance meeting their needs with being present with your newborn. Many mothers have to leave hospital long before their baby is ready to come home and have to travel back and forwards to be with their baby. This is a time to say yes to as many offers of help as you possibly can. If someone can provide a lift, deliver a meal, entertain an older child or do a load of washing – or just sit with you to talk things over in the hospital cafe – these may make life a little easier for you and help you to keep going at a difficult time.
You may be taking medications yourself and be concerned about them passing through your milk. Discuss your concerns with your and your baby’s medical teams. They may be able to reassure you or find suitable alternatives. For specialist information about whether a drug is compatible with breastfeeding, you can contact your local LLL Leader who has access to resources and professional support.
It may feel impossibly painful to keep leaving your baby. Remember that by looking after yourself – eating, sleeping and taking the medication you need to get well – you are making sure that you carry on being able to be there to look after your baby.
Taking your breastfed baby home
Separately to any health issues your baby may be facing, your neonatal unit will want to know that you are able to make sure your baby is getting enough milk to continue growing. Being aware of your baby’s early hunger cues is important so that you can feed responsively and before baby gets too upset. You may have a very sleepy baby who still needs your help to wake themselves up to feed beyond their due date. Setting an alarm for the middle of the night can help you to make sure they don’t go for longer than a four hour stretch without feeding at night.
Read more about recognising early hunger cues and about waking a sleepy baby here.
Read more about how to tell if your baby is getting enough milk here.
Many breastfeeding mothers and babies enjoy safe cosleeping. Premature babies are at greater risk of Sudden Infant Death Syndrome or Sudden Unexplained Death in Infancy (SIDS/SUDI). While they will benefit from sleeping close to their mother, premature babies should sleep on a separate, firm surface such as a sidecar cot.
It can be scary to make the transition from caring for your baby in hospital with a team of staff around you, to being at home. Your healthcare professionals are likely to make extra visits to support you and to keep an eye on your baby’s weight gain. You may find that being home together, able to stay together all the time, and in a comfortable environment, you rapidly get to know and understand your baby more easily and become more confident in your mothering skills.
Photo credits: Olivia Brown and other mothers
Other resources
You can read a mother’s story about mothering her premature baby through special care
This video looks at breastfeeding in the first hour after birth
The drugs in breastmilk service, while not an LLL resource, gives quick access to information from a qualified pharmacist
The Small Wonders films follow families through their experiences of having a baby on a neonatal unit
Global Health Media have a series of videos about various aspects of life with a small baby