Are you experiencing pain while breastfeeding, possibly combined with slow weight gain for your baby? While the vast majority of such breastfeeding problems can be resolved by adjusting positioning and attachment, and with good breastfeeding management, occasionally tongue tie might be the cause of the problem.
Tongue tie (ankyloglossia) is caused by a tight or short lingual frenulum (the membrane that anchors the tongue to the floor of the mouth). The frenulum normally thins and recedes before birth. Where this doesn’t happen, the frenulum may restrict tongue mobility. Tongue tie often runs in families and is thought to be more common in boys than girls. There is an association between high or unusual palates and tongue tie, because restricted tongue movement can affect the shape of the palate.
Breastfeeding challenges can also occur for other reasons. Identifying the cause is important when deciding on appropriate solutions, so seek help from someone skilled.
Identifying tongue tie
When your baby tries to lift their tongue or move it forwards it may appear misshapen, short or heart-shaped, with the frenulum clearly pulling its centre down and restricting its movement. Or you may be able to see or feel firm tissue where their tongue meets the floor of his mouth. Degrees of tongue tie vary and it can be difficult to diagnose accurately. A short, tight, posterior tongue tie is rarer, but may be particularly hard to spot.
How breastfeeding may be affected
Tongue tie affects tongue movement to varying degrees. The shorter and tighter it is, the more likely it is to affect breastfeeding. Some babies with a tongue tie breastfeed well from the start, others do so when positioning and attachment are improved. But any tongue tie that restricts normal tongue movement can lead to breastfeeding difficulties. A baby needs to be able to move their tongue freely and extend it over the lower gum with their mouth open wide to be able to breastfeed well. The symptoms below are all associated with poor attachment that may be caused by tongue tie.
A baby may:
• Be unable to latch on to the breast at all.
• Be unable to latch on deeply, causing nipple pain and damage.
• Have difficulties staying on the breast, making a clicking sound as he loses suction.
• Splutter and choke when coping with fast flowing milk.
• Breastfeed constantly to get enough milk.
• Have poor weight gain or need supplementation to maintain adequate weight gain.
• Develop jaundice that needs treating.
• Be fussy at the breast when the milk flow slows.
• Develop colic.
A mother may experience:
• Pain during feeds, with damaged nipples. Her nipple may be compressed or distorted into a wedge shape like that of a new lipstick immediately after feeding, often with a stripe at its tip.
• Engorgement, blocked ducts and mastitis because of ineffective milk removal.
• Low milk production because of ineffective milk removal.
• Oversupply—if her baby compensates for not being able to breastfeed well by nursing very frequently.
• Tiredness, frustration and discouragement.
• A premature end to breastfeeding.
Breastfeeding is important for every baby
Though sometimes needed as a temporary supplement if your milk production is very low, introducing infant formula is not the answer. It has short-term and long-term health risks for both your baby and you. A baby with tongue tie can also have difficulties with bottlefeeding. Milk may leak from his mouth during feeds and he may suffer from colic.

Treatment
Where a tongue tie is causing breastfeeding problems, treatment options are available and effective— especially if the treatment is prompt. Although attention to positioning and attachment can help maintain breastfeeding and improve comfort to a certain extent, there is evidence that treating tongue tie by frenotomy (see below) is effective in resolving breastfeeding difficulties. Weight gain can improve dramatically. As well as the continued breastfeeding benefits, continuing to breastfeed after frenotomy maximises a baby’s chance of normal mouth (palate), speech and dental development. This includes tongue mobility for licking and moving particles of food around the mouth, helping prevent tooth decay.
Keeping breastfeeding going
Mastering the art of breastfeeding can sometimes be a challenge and it takes determination to keep going if you are in pain. The information here can help you keep breastfeeding, both before and after treatment.
Soften your breast
A baby with tongue tie may find it easier to latch on if your breast is soft so breastfeed frequently to avoid engorgement. When your baby bobs their head and licks the nipple, they naturally makes it easier to latch on. Or you can use reverse pressure softening to move fluids away from the nipple area so your baby can latch on well. Press all five fingertips of one hand around the base of the nipple. Apply gentle steady pressure for about a minute to leave a ring of small dimples on the areola. You can also press with the sides of your fingers. Place your thumb on one side of the nipple and two fingers on the other side where your baby’s lips will be. Gently hand express a little milk if needed.
Biological nurturing™
A baby often instinctively attaches more deeply and comfortably if they can snuggle up close to their mother’s chest for periods of time. Try letting your baby lie on your body as you recline so both their chest and tummy are against you. This kind of ‘laid-back’ breastfeeding contact is known as Biological Nurturing™ and can be done skin-to-skin or with you and your baby lightly clothed—whatever is more comfortable and convenient for you both. Because gravity helps a baby keep their tongue forwards, this can make a real difference to how well your baby feeds and how much milk you make. See picture above and Online Information section for details of an online video.
A deeper latch
Help your baby get as deep a latch as possible at the breast. This will maximise the amount of milk they get and minimise nipple pain.
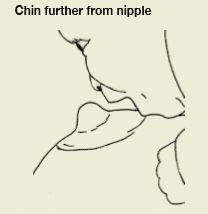
If your baby retracts (pulls back) their tongue when they open their mouth, try sliding their chin a little further from the nipple so he can feel the ‘fatter’ part of the breast with his tongue. Denting the breast at the edge of the areola with a finger and placing your baby’s chin in the dent may also help.
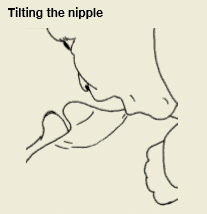
You could also try placing your thumb or finger near the base of the nipple where your baby’s upper lip will be. If you press, your nipple will tilt away from your baby, presenting them with your breast rather than your nipple. As they open wide, snuggle them in close and use your thumb or finger to tuck the breast into their mouth. Your nipple will be taken in last and unroll in their mouth. If needed, you can then slip your finger out. An LLL Leader can give you further suggestions to help you improve your baby’s positioning and attachment
Encourage tongue mobility
To encourage your baby to move their tongue forward, you can also try:
• Reclining with your baby on top of you. Try leaning forward and back yourself to understand how gravity affects tongue position.
• Encouraging them to lick milk from their lips or from your nipple before and after feeds.
• Sticking your tongue out at your baby to encourage them to copy you.
Maintain milk production
If your baby is sleepy or has jaundice, or if you have engorgement or inverted nipples, then a tongue tie can make things worse. If they are not able to take enough milk directly at the breast then you will need to express it and give it to your baby until they are able to breastfeed effectively. Express by hand and/or with a pump at least 8 times a day if your baby is not draining the breast well. This will maintain your milk production and ensure they get enough milk.
Small amounts of expressed milk can be offered by spoon, cup or syringe while you both learn how to breastfeed. Bottles or dummies can confuse your baby’s sucking technique so consult an LLL Leader about breastfeeding friendly ways to bottlefeed or about using a nursing supplementer. This device delivers extra milk through a tube along your breast as your baby nurses, avoiding the need for bottles.
An unusual palate
Restricted tongue movement caused by tongue tie may affect the shape of a baby’s palate, leading to a high palate or a bubble palate with a high spot. These may be a factor in broken suction, a clicking sound and pain during breastfeeding. A baby with an unusual palate may also resist a deeper latch due to gagging.
The following may help.
• Start with a clean finger with closely trimmed nail.
• Touch your baby’s lips and wait until they open their mouth.
• Gently slide in your finger, pad side up along his hard palate, stopping just before the gag reflex is triggered.
Make this a pleasant game and, over a few days, gradually move your finger back to overcome sensitivity. After a tongue tie is divided, a baby’s increased tongue movement helps the palate shape become more normal
Treating Tongue Tie
What can be done?
Frenotomy—dividing the tongue tie—can dramatically improve breastfeeding comfort and efficiency for both mother and baby. Dividing a tongue tie is a quick and simple procedure. No anaesthetic is needed for a baby under six months of age.
There are health professionals around the UK who have been specifically trained to divide tongue ties. For treatment on the NHS, you will need a referral from your midwife, health visitor or GP. Knowledge about tongue ties and how they affect breastfeeding varies, so it is worth persisting and seeking a second opinion. In areas where only GPs can refer, your midwife or health visitor may be able to give a recommendation to your GP or suggest seeing a particular GP. Private treatment may also be an option. See Further Reading for information on finding a practitioner trained to divide tongue ties
Is waiting an option?
Sometimes a very thin tongue tie breaks spontaneously or can be stretched by gentle massage of the frenulum. The earlier a tongue tie is divided, the easier it is to resolve any breastfeeding difficulties. Dividing a tongue tie in a baby over six months old is also a more complicated procedure and usually requires a general anaesthetic.
Frenotomy—what will happen?
After the health professional’s initial assessment, your baby will be swaddled and held (often by an assistant) so they stay still during the procedure, which only takes a minute or two. The health professional lifts the tongue and divides the frenulum by cutting it with a pair of round-ended sterile scissors or by cauterising it.
Does it hurt?
No anaesthetic is needed for a very young baby as having a tongue tie divided only hurts a little, if at all. Some babies protest more at being swaddled than about the treatment. Others sleep right through the procedure! You will be asked to breastfeed your baby as soon as the procedure is over, to offer comfort, clean the wound and get their tongue moving as soon as possible. The inside of a baby’s mouth heals very quickly. The only treatment usually needed is to breastfeed to keep the wound clean and keep his tongue mobile. There may be a white patch under your baby’s tongue, but this heals within 24 to 48 hours.
If things don’t resolve
Usually a mother notices an instant improvement in her comfort during breastfeeds. Sometimes it takes a week or two for a baby to adjust to their tongue’s greater mobility. An older baby may find it harder to adjust to increased tongue mobility and tongue exercises may be recommended. Occasionally a baby’s frenulum needs dividing a second time, usually because the division was not quite extensive enough the first time. If you suspect that the initial procedure has not resolved your baby’s breastfeeding problems arrange another consultation. Do persist with finding solutions. If several factors are involved it can take time and expertise to resolve the problem. An LLL Leader can suggest further paths to explore and provide ongoing support.
Painful nipples
Using different feeding positions can help if breastfeeding is painful. Or use the position you find most comfortable until your nipples heal. Check your baby’s attachment later in the feed—if they slip down your nipple, this may cause you pain. Reclining breastfeeding positions or extra support under your arms may help.
Ask your LLL Leader about breast compression, which can help your baby get more milk quicker. An increase in milk flow may also help them breastfeed more effectively.
Hand express to stimulate milk flow before feeding. Or start on the least painful side, switching sides once your milk lets down. Pain can reduce milk flow, leading to engorgement and mastitis. Ask your doctor, midwife or health visitor about using a suitable painkiller. Applying warmth and using gentle massage and relaxation exercises just before feeds can help milk to flow.
Moist wound healing
When the underlying problem is corrected, moist wound healing can help your nipples heal without scab formation. After each feed gently pat your nipples dry to remove surface wetness. Apply a tiny smear of ultra pure modified lanolin to each nipple, dabbing it on rather than rubbing. Hydrogel pads without a cloth backing can also be used.
Blood from cracked nipples
Blood from cracked nipples is not harmful to your baby. You can continue to breastfeed whilst working to improve positioning and attachment.
If healing is slow
Once your baby starts latching on well you should feel more comfortable and notice signs of healing within a few days. If not, visit your GP—sometimes a bacterial or fungal infection can prevent healing. Continued pain may be a sign that treatment (or further treatment) of your baby’s tongue tie is needed.
Seek support
This is a time when the support of other mothers in your local LLL group can be invaluable. You can find your nearest Leader or by calling our Helpline.
Further Reading
Find a tongue tie practitioner– Association of Tongue Tie Practitioners, has details of both NHS and Private Practitioners
Biological Nurturing™
Lactation Consultants of Great Britain
The Womanly Art of Breastfeeding. LLLI. London: Pinter & Martin, 2010: p63-81, 428-430.
Comfortable Breastfeeding
Engorged Breasts – Avoiding & Treating
Expressing Your Milk
Hand Expression of Breastmilk
My Baby Needs More Milk
Nipple Know-How
Nipple pain
Nursing Supplementers
Sleep Baby – Why and What To Do
Storing Your Milk
LLLI Resources
Tongue Tie & the Breastfed Baby
References
Hazelbaker, AK. Tongue-Tie: Morphogenesis, Impact, Assessment and Treatment. Columbus, OH: Aidan and Eva Press, 2010.
Mohrbacher, N. Breastfeeding Answers Made Simple. Amarillo Tx: Hale Publishing, 2010.
Watson Genna, C. Supporting Sucking Skills in Breastfeeding Infants. Burlington, MA. Jones & Bartlett, 2012.
Geddes, DT. et al. Frenulotomy for breastfeeding infants with ankyloglossia: Effect on milk removal and sucking mechanism as imaged by ultrasound. Pediatrics 2008; 12(1):e188–94.
Hogan, M. Westcott, C. and Griffiths, M. Randomized, controlled trial of division of tongue-tie in infants with feeding problems. J Paediatr Child Health 2005; 41:246–50.
Hong, P. et al. Defining ankyloglossia: A case series of anterior and posterior tongue ties. Int J Ped Otorhinolaryngology 2010; 74:1003–6.
Knox, I. Tongue tie and frenotomy in the breastfeeding newborn. Neoreviews 11 (9) Sept 2010.
Miranda, BH. and Milroy, CJ. A quick snip—a study of the impact of outpatient tongue tie release on neonatal growth and breastfeeding. JPRAS 2010; 63:e683–5.
Watson Genna, C. And Coryllos, EV. Breastfeeding and tongue-tie. J Hum Lact 2009; 25(1):111–2.
You can buy this information in printed form from the LLLGB Shop.
Copyright LLLGB 2016